
Cloud EHR vs On-Premises EHR: The Ultimate Comparison
For most healthcare organizations, the Cloud EHR is no longer a “risky new option”; it is the operating model that best aligns with modern clinical workloads, cyber risk realities, and regulatory expectations around demonstrable governance. In regulated healthcare, the key question is less whether cloud can be compliant, and more whether your organization can consistently engineer and sustain the same level of resilience, security monitoring, patch velocity, and disaster‑recovery readiness on‑premises without ballooning cost and complexity.
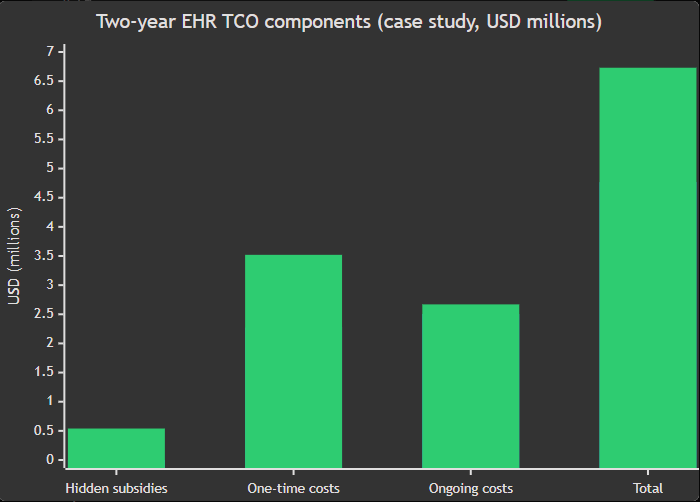
A peer‑reviewed case study comparing an on‑premises EHR upgrade versus a cloud‑based EHR deployment in a healthcare education clinic found the two‑year total cost for on‑premises was US$6.73m versus US$4.76m for cloud, a difference of ~US$1.97m. The same study surfaced “hidden subsidies” borne by on‑premises (facilities/energy, disaster recovery readiness, business continuity response) totalling US$539,908, while those costs were US$0 in the cloud scenario.
Meanwhile, EHR adoption is effectively mainstream (for example, 95.0% of U.S. office‑based physicians reported EHR adoption in 2024, and 83.6% reported using a certified EHR). Once EHRs are ubiquitous, competitive advantage shifts to how well the platform supports interoperability, remote care, rapid improvement cycles, and resilient operations.
Cloud EHR is not automatically “more secure” by definition. However, official guidance in both the U.S. and UK frames cloud as compatible with healthcare obligations when governance is done correctly (e.g., HIPAA allows cloud use with appropriate contracts and risk management; the NHS promotes a cloud‑ and internet‑first default model and publishes detailed cloud security and data guidance).
Introduction and assumptions
Assumptions (explicitly unspecified by the requester): organization size (single site vs multi‑site), care setting (acute, ambulatory, dental, mental health), budget constraints, current EHR vendor, current hosting model, network maturity, and the primary regulatory jurisdiction(s). The comparison, therefore, focuses on principles and widely applicable regulatory patterns in the UK/EU (GDPR/UK GDPR) and the U.S. (HIPAA), plus generally accepted cloud risk concepts from standards bodies.
What “Cloud EHR” means in practice. In healthcare procurement, “cloud” typically spans:
- SaaS EHR (vendor operates the full application; the subscriber configures and governs use),
- hosted/managed EHR on cloud infrastructure, and
- IaaS/PaaS deployments where your organization (or a partner) retains more technical control.
Using the National Institute of Standards and Technology definition, cloud computing is characterized by on‑demand self‑service, broad network access, resource pooling, rapid elasticity, and measured service, properties that map directly to healthcare needs such as surge capacity (winter pressures), multi‑site access, and predictable service management.
Related: Cloud EHR for Specialty Clinics: Full Guide (Features, Benefits, Pricing, Integrations)
Cloud vs on‑premises analytical comparison across key dimensions
The summary below synthesizes primary guidance and evidence from healthcare regulators, UK/NHS cloud guidance, and standards bodies; cost metrics include a peer‑reviewed two‑year EHR TCO comparison.
| Dimension | Cloud EHR (typical reality) | On‑premises EHR (typical reality) |
| Cost model | Opex‑leaning subscription + implementation + integration; costs scale with use; less capital outlay. | Capex‑heavy (infrastructure + refresh cycles) plus ongoing staffing/operations; “hidden subsidies” are common. |
| Security posture | Can meet HIPAA/UK/NHS expectations with the right contracts, risk analysis, encryption, and shared‑responsibility clarity. | Full responsibility sits with your organization; security depends on sustained maturity (patching, monitoring, resilience engineering). |
| Compliance execution | Strong audit artifacts are often easier to evidence (central logging, standardized controls), but you must govern vendor + transfers. | Compliance is fully internal; easier to achieve local physical control, harder to sustain enterprise‑grade assurance at scale. |
| Scalability & performance | Elastic scaling; better fit for analytics/AI‑adjacent workloads and variable demand. | Scaling often means procurement + build time; performance can be strong locally, but harder to expand across sites. |
| Implementation & maintenance | Faster environment provisioning; vendor handles more upgrades/patching in SaaS models; organizational work shifts to change management and workflow design. | More control over timing, but more internal burden (hardware lifecycle, OS/database administration, patch windows). |
| Interoperability & integrations | API‑first patterns align well with FHIR ecosystems and nationwide frameworks like TEFCA; they still require governance and interface engineering. | Integrations can be robust but often slower to modernize; interface engines and upgrades become local responsibilities. |
| Disaster recovery & continuity | Multi‑site resilience can be engineered more economically; it still must meet contingency plan obligations and be tested regularly. | Often expensive to do well (secondary sites, replication, DR tooling, power/cooling); frequently under‑funded until an incident occurs. |
| UX & accessibility | Better supports web/mobile access and remote workflows; dependence on network availability must be mitigated. | Can be excellent on‑site; remote/mobile access often needs additional infrastructure and cost. |
| Customisation & control | Configuration‑heavy rather than code‑heavy; SaaS shifts control/risk to the provider; some deep customizations may be constrained. | Maximum technical control; supports niche legacy dependencies, but increases operational risk and upgrade friction. |
| Lock‑in & migration | Lock‑in risk is real in SaaS; it can be mitigated via contract terms, export formats, integration abstraction, and portability planning. | “Lock‑in” shifts from vendor to your own environment (custom interfaces, bespoke infra); migrations can be equally hard, just in different ways. |
Cost and total cost of ownership
The most persuasive pro‑cloud argument for decision‑makers is not “cloud is cheaper”, it is that cloud makes full cost visible and reduces the tendency for critical reliability/security work to become unfunded “background subsidies”.
A peer‑reviewed EHR TCO comparison found two‑year totals of US$4,762,871 (cloud) vs US$6,731,715 (on‑premises). The on‑premises scenario carried explicit “hidden subsidies” (facilities/energy US$239,908, disaster recovery readiness US$200,000, business continuity response US$100,000).
The itemization is operationally revealing: on‑premises required materially more spending on staffing, reporting, and remote/mobile access enablement, while cloud concentrated spend into subscription/licensing plus support and functional teams.
This is exactly the strategic shift Cloud EHR enables: fewer fragile infrastructure costs; more spend on outcomes (adoption, workflow, safety).
Bar chart (case study): two‑year TCO components (US$ millions).
Security and compliance
A cloud deployment does not change your legal accountability; it changes how you fulfil it. That is a feature, not a bug, because it forces explicit contracts, clearer responsibility boundaries, and repeatable control frameworks.
For HIPAA, the U.S. Department of Health and Human Services guidance explicitly states that a HIPAA-covered entity or business associate may use cloud services to store/process ePHI, provided a HIPAA‑compliant Business Associate Agreement is in place, and the organization otherwise complies with the HIPAA Rules. It also clarifies that a cloud service provider is a business associate even if it only stores encrypted ePHI and does not hold the decryption key.
HIPAA’s Security Rule is risk‑based: regulated entities must conduct a risk analysis and implement administrative/physical/technical safeguards to protect confidentiality, integrity, and availability. Contingency planning (data backup, disaster recovery, emergency operations) is a defined administrative safeguard.
For GDPR/UK GDPR, the compliance “trap” in cloud EHR is rarely encryption; it is governance: defining controller/processor roles, ensuring Article 28‑grade contracts, carrying out DPIAs where required, and managing international transfer risk where cloud operations or support create “restricted transfers.”
The European Data Protection Board’s coordinated enforcement report on public‑sector use of cloud services highlights recurring challenges around controller‑processor arrangements and international transfers post‑Schrems II, and points to “leading practices” including deeper contract assessment/renegotiation with close DPO involvement.
Data residency. NHS England cloud data guidance states a direction that NHS data at rest remains within the UK, encrypted at rest (minimum AES‑256) and encrypted in transit (TLS 1.2 as default). It also notes that some processing may occur in Europe (GDPR‑covered) where needed, but requires a DPIA and approvals for workloads that transmit data outside the UK for processing.
Finally, modern cloud security is explicitly framed as shared responsibility: the National Cyber Security Centre describes the shared responsibility model as a way to clarify who secures what and argues organizations should cede as much security responsibility as sensible to trusted providers, while still governing identity, configuration, and data.
Related: Evaluating Cloud vs On-Premises EHR: TCO, Security, and Workflow Impact for 2026 Buyers
Scalability and performance
Cloud’s performance advantage in EHR is less about “faster servers” and more about elasticity and operational predictability during peaks: seasonal demand, outbreaks, large‑scale reporting, and analytics expansion.
NIST’s definition highlights “rapid elasticity” and “resource pooling,” which map well to multi‑site health systems and variable workloads. In the NHS context, cloud policy frames public cloud as enabling flexibility for winter pressures and large‑scale responses, and as reducing risks tied to ageing hardware and refresh cycles.
Balanced view: Cloud increases dependency on networks and providers. NIST’s cloud computing recommendations explicitly discuss network dependence and cloud provider outages as open issues, meaning resilience design (offline procedures, downtime modes, local caching where appropriate) must be intentional.
Implementation and maintenance
Implementation success correlates more with change management than with hosting model, but cloud materially improves the engineering economics of applying updates, scaling environments, and standardizing operational tooling.
The NHS cloud migration guidance explicitly positions “SaaS‑first” as a common approach because SaaS delivers many cloud benefits with lower barriers, while acknowledging that SaaS shifts control and risk to the provider (which some organizations may not accept).
This trade‑off shows up in cost accounting: the peer‑reviewed TCO study includes on‑premises costs for system administration staff and application/database administration that were not present in the cloud scenario, while cloud had higher subscription/licensing and migration/training emphasis.
Crucially, safety bodies warn that EPR implementation is complex and must engage users, manage configuration risk, and align upgrades with clinical risk management standards. Cloud makes upgrades easier, but does not eliminate the need for clinical safety governance.
Interoperability and integrations
Interoperability is where Cloud EHR can become a strategic accelerator, not because cloud magically “integrates,” but because cloud architectures tend to align with modern API standards and integration patterns. HL7’s FHIR standard is a widely adopted framework for exchanging healthcare information electronically, and UK interoperability guidance points to FHIR‑based approaches for consistent information flows. In the U.S., TEFCA provides a nationwide framework intended to reduce barriers to electronic health information sharing.
Yet the data shows the work is unfinished: in 2023, only 43% of U.S. hospitals reported routinely engaging in all four domains of interoperable exchange, even though broader engagement is higher.
A cloud‑friendly, API‑first EHR strategy (plus a disciplined integration layer) is one of the most practical ways to close that gap without continually rebuilding bespoke interfaces.
Disaster recovery and business continuity
Healthcare is now firmly in the era where cyber disruption is a patient‑safety risk, not just an IT problem.
HIPAA’s administrative safeguards explicitly require contingency planning, including disaster recovery and emergency mode operation planning. NIST’s contingency planning guidance formalizes concepts like recovery time objectives and recovery point objectives, which should drive the design of EHR downtime procedures and restoration plans regardless of hosting.
From an economic perspective, the peer‑reviewed EHR TCO study is blunt: on‑premises carried explicit DR readiness and business continuity costs inside “hidden subsidies,” while cloud did not.
Cloud doesn’t eliminate DR engineering; it makes resilient patterns (multi‑site replication, automated backups, infrastructure redundancy) more attainable for organizations that would otherwise under‑invest.
User experience and accessibility
Cloud’s “broad network access” property (NIST) directly supports clinical realities: ward mobility, community care, multi‑site access, and remote working.
Cost evidence again illustrates the practical difference: the case study assigned US$550,000 (two‑year) to “remote and mobile access” for on‑premises versus US$0 for cloud, implying that enabling secure mobility can be significantly more expensive when you must build and maintain the supporting infrastructure yourself.
Balanced view: increased reliance on internet connectivity must be addressed through clinical downtime planning and resilient network design; cloud migrations should treat the network as a clinical dependency.
Customization and control
On‑premises EHR is often chosen for perceived control: direct access to servers, bespoke integrations, and one‑off custom workflows. In reality, this “control” frequently becomes control over legacy constraints.
NHS guidance is explicit that cloud‑first does not mean every workload must move to the cloud; on‑premises may still be right where cloud cannot meet specific regulatory or latency requirements.
The persuasive cloud position is therefore: prefer configuration over custom code. Choose a Cloud EHR that supports clinical configuration safely (templates, order sets, dictionaries, workflow rules) and reserve deep custom development for areas where it is truly differentiating, you accumulate upgrade blockers and safety risk through local change.
Vendor lock‑in and migration
Lock‑in is a valid concern, and it is frequently mishandled by treating it as purely technical. The UK government’s cloud guide defines lock‑in as dependency that makes switching difficult, time‑consuming, and disproportionately expensive; it also clarifies that “overseas hosting” includes not only physical location but also who manages and can access the data.
NIST also flags portability problems, notably “lack of portability between SaaS clouds,” reinforcing that exit planning must be designed, not wished for. That said, on‑premises is not “lock‑in free”: custom interfaces, brittle infrastructure, and institutional knowledge trapped in local teams are a form of self‑inflicted lock‑in, often with worse resilience. The right decision is to choose the cloud, then design for exit.
Real‑world examples and case studies
Peer‑reviewed cost case study. University of Michigan School of Dentistry compared upgrading an on‑premises EHR to deploying a cloud‑based EHR using a total cost of ownership framework. The on‑premises option was ~US$1.97m higher over two years, and carried hundreds of thousands in facilities/energy and DR/BC costs that were not present in the cloud scenario.
National direction of travel. NHS cloud policy explicitly frames public cloud and “internet first” as the default delivery model, while allowing exceptions. Separately, NHS England’s frontline digitization programme notes £1.9bn invested to raise baseline digital capability and states 95% of trusts are expected to have implemented or upgraded an EPR by March 2026. This institutional momentum matters: it shapes supplier roadmaps, workforce skills, and procurement norms toward cloud‑compatible delivery.
A vendor example of cloud‑operated EHR at scale. MEDITECH describes “MEDITECH as a Service” as a subscription model delivered with capabilities of Google Cloud Platform, and states its MaaS customer base surpassed 100 sites across multiple countries. While vendor material should be read as directional rather than neutral, it illustrates that “cloud EHR” is now a mainstream commercial delivery path rather than an edge case.
A necessary caution. The Health Services Safety Investigations Body thematic review notes EPR systems can contribute to missed, delayed, or incorrect care when capabilities, usability, configuration, governance, and optimization are weak, reinforcing that cloud migration must be paired with a rigorous clinical safety and adoption strategy.
Best‑practice migration playbook
A Cloud EHR migration is best treated as a clinical transformation programme with a technology backbone, not a hosting refresh. UK/NHS guidance is explicit about workload assessment, placement strategies (including the “5 Rs”), and cloud tier choice; U.S. HIPAA guidance emphasizes contracts (BAA), risk analysis, and SLAs covering availability/backup and data return. EU/UK GDPR guidance emphasizes DPIAs, controller‑processor contracts, and transfer risk management.
Pre‑migration checklist for decision‑makers
Establish a single accountable executive owner and governance forum that includes clinical safety, information governance/privacy, cybersecurity, operations, and finance.
Confirm your target cloud tier (SaaS‑first where feasible) and document the rationale for exceptions (latency, regulation, legacy dependency).
Define and test downtime procedures (clinical workflows, RTO/RPO targets, and contingency plan evidence) before go‑live.
Treat vendor contracts as security controls: include audit/assurance artifacts, breach notification obligations, backup/restore responsibilities, and clear data return/portability terms.
For UK/NHS contexts, ensure data at rest, encryption, and processing location assumptions match published NHS cloud data guidance; for cross‑border processing, ensure DPIA and approvals.
Risk mitigations that materially reduce failure modes
- Connectivity risk: design for network dependency, because cloud EHR availability is constrained by network reliability.
- Cyber disruption: align ransomware readiness with contingency planning requirements. EU health‑sector incident patterns show ransomware remains a dominant threat signal.
- Configuration safety: implement clinical safety governance for templates, order sets, and workflows; both patient safety literature and national safety reviews flag configuration and optimization as recurring risk points.
- Portability and exit: require export mechanisms, time‑bounded data return, and interoperability safeguards; NIST highlights portability issues between SaaS clouds, making this a first‑class design concern.
Cost considerations that prevent “cloud sticker shock.”
Anchor your business case in the total cost of ownership, not just the subscription price. Explicitly surface costs that are often ignored in on‑premises models (facilities/energy, DR readiness, business continuity response, and the true staffing footprint). The peer‑reviewed EHR TCO study demonstrates how large these “unpriced” categories can be.
Budget for adoption and safety, not only technology. Patient safety guidance emphasizes training, incident learning, and governance as core to safe EPR implementation, areas that often become underfunded when the focus is purely on hosting.
Conclusion
If you are deciding purely on “where the servers sit,” you will miss the real strategic question: which model gives your organization the highest probability of sustaining safe, compliant, resilient, continuously improving clinical operations over the next decade.
The evidence and guidance trend in the same direction. Standards bodies frame cloud as a model built around elasticity and broad access; regulators permit cloud use when governance is correct; NHS policy treats cloud and internet‑first as the default; and real EHR cost evidence shows on‑premises can carry substantial hidden costs that cloud models bring into the open.
Cloud EHR is therefore the stronger default choice for most healthcare IT leaders, provided you pair it with rigorous clinical safety governance, contract discipline, and an exit‑ready architecture.
Frequently Asked Questions
1. What are the key differences between cloud EHR and on-premises EHR systems?
Cloud EHR runs on vendor-managed servers with a subscription model, offering remote access, automatic updates, and lower upfront costs. On-premises EHR is hosted on your own servers, requiring dedicated IT infrastructure and higher capital investment. For most practices, cloud-based EHR delivers better scalability, lower total cost of ownership, and easier compliance management.
2. What are the cost comparisons for cloud EHR versus on-premises EHR implementations?
Cloud EHR typically costs less over time. A peer-reviewed study found cloud EHR had a two-year total cost of approximately $4.76 million versus $6.73 million for on-premises, a difference of nearly $2 million. On-premises systems carry high hidden costs, including facilities, disaster recovery readiness, and IT staffing, which cloud EHR pricing models fold into a transparent monthly subscription.
3. What IT expertise is needed to manage a self-hosted EHR?
Managing a self-hosted on-premises EHR typically requires dedicated IT staff skilled in server administration, database management, network security, and HIPAA compliance. You’ll also need expertise in patch management, disaster recovery planning, and hardware lifecycle maintenance. In contrast, cloud EHR shifts most of this burden to the vendor, making it far more manageable for small and mid-sized practices with limited IT resources.
4. What are the ongoing monthly fees for popular cloud EHR platforms?
Monthly EHR pricing for cloud platforms varies widely by vendor and features. Vozo EHR starts at $25/month, Practice Fusion at $149/month, and AdvancedMD at $229/month per provider. Always verify what is included in the base price, as add-ons like telehealth, e-prescribing, and patient engagement tools are often billed separately, significantly increasing the total monthly cost.
5. What are the pros and cons of cloud-based versus on-premise EHRs?
Cloud EHR offers lower upfront costs, automatic updates, remote access, and built-in disaster recovery, making it ideal for most modern practices. On-premises EHR provides maximum control and deep customization but comes with high capital costs, IT overhead, and hidden expenses around security and maintenance. For most small to mid-sized practices, cloud-based EHR delivers stronger long-term value and operational resilience.
Vozo EHR for your Healthcare Practices
From managing and organizing patient health records digitally to reducing medical errors, it significantly empowers providers to improve healthcare quality.
If you are searching for the best EHR system for your healthcare practice, Vozo EHR can be your go-to choice. Our comprehensive EHR solution lets you focus more on patient care while carrying all the burdens and simplifying it.
- Vozo Cloud EHR’s cost-effective cloud subscription benefits all levels of practice.
- Our feature-rich EHR helps you rectify mistakes efficiently and speed up the process.
- Vozo Specialty EHR resonates with specialty practice needs and requirements.
- Our expert technical team has got you covered 24/7 if any needs arise.
- Our EHR System continues to scale as your healthcare practice grows to improve the user experience.
The Vozo Customized EHR solution benefits your healthcare practice by:
- Streamlining the administrative process
- Improving workflow efficiency
- Reducing proneness to errors
- Managing all the patients’ records in one place
- Offers greater efficiency and cost savings across the board.
Our specialty-specific tools, such as scheduling, patient portals, lab integration, cloud hosting, and more, meet the specific needs and requirements of your healthcare practice.
“Embrace Vozo EHR to reduce your burdens and enhance patient care”.
About the author
Lara Dixit

Lara Dixit is a Senior Business Manager at Vozo Health, specializing in EHR platforms, practice management, billing, and revenue cycle optimization. She helps healthcare providers improve operational efficiency, streamline workflows, and drive sustainable practice growth. At Vozo Health, she focuses on business strategy, healthcare automation, and scalable growth for modern medical practices.









