
What Are GIRP Notes? A Goal-Focused Format Explained
Therapy notes often fail in one of two ways.
They either record so much detail that the treatment logic becomes difficult to find, or they record so little that another provider cannot tell what the session accomplished.
The GIRP note format offers a middle ground.
By organizing each progress note around the client’s Goal, the clinician’s Intervention, the client’s Response, and the Plan, GIRP notes make the relationship between treatment objectives and session activity easier to follow.
But GIRP is not simply four headings to complete.
A useful GIRP note should explain why the service was provided, what clinically relevant action was taken, how the client responded, and what should happen next.
Key Takeaways
- GIRP (Goal, Intervention, Response, and Plan) is a structured format for writing therapy progress notes that is directly connected to the client’s plan of care.
- GIRP can be useful in goal-driven programs because its structure makes the relationship between the plan of care, intervention, client response, and next step easier to review.
- Each section serves a specific purpose: Goal is to focus the session, Intervention is to record what you did, Response is to record what happened, and Plan is to drive what will happen next.
- GIRP is not the right fit for every session. Crisis presentations, insight-oriented modalities, and vague treatment plans all call for a different approach.
- The most common GIRP documentation mistakes, loose goal paraphrasing, vague intervention language, and thin response notes, are entirely preventable with the right workflow.
- A behavioral health EHR with structured GIRP templates can help reduce missing fields and improve documentation consistency.
What Are GIRP Notes?
GIRP notes are goal-focused behavioral health progress notes divided into four sections: Goal, Intervention, Response, and Plan. Mental health professionals use the format to connect each session to the client’s plan of care, document the techniques used, describe the client’s response, and establish clear next steps for care.
- Goal: The specific objective from the client’s plan that the session addressed
- Intervention: What the clinician actually did during the session
- Response: How the client reacted to that intervention
- Plan: What happens next, for the client and for treatment overall
Each section answers a different question a payer, supervisor, or future treating clinician might ask when reading the chart.
Together, they tell a complete, ordered story: here’s what we were working toward, here’s what I did about it, here’s how the client responded, and here’s where we go from here.
GIRP is widely used across outpatient therapy, community mental health centers, intensive outpatient programs, and group practice settings, particularly where treatment plan compliance is closely monitored.
Related Blogs: What Are BIRP Notes? How to Write Them Step by Step
Breaking Down the GIRP Note: Section by Section
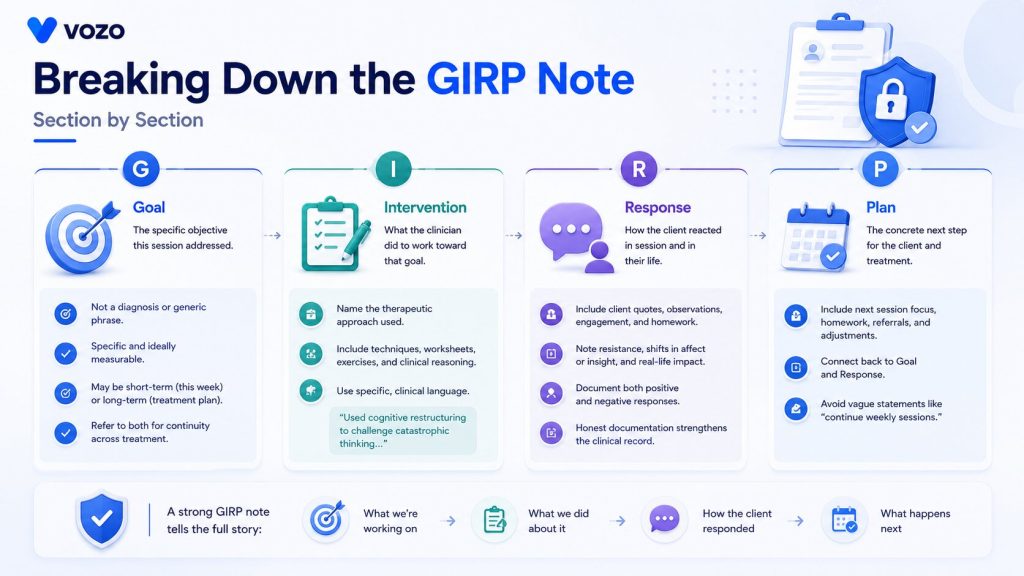
Goal
The Goal section names the specific objective this session addressed.
This isn’t a restatement of the client’s diagnosis or a generic phrase like “improve coping skills.” A strong Goal section points to something specific and ideally measurable, such as reducing panic attack frequency, building tolerance for a feared social situation, or strengthening a particular coping skill the client has been working on across sessions.
Goals may be short-term (this week’s focus) or long-term (broader treatment plan target), and many clinicians refer to both of these, which makes for continuity throughout the entire course of treatment.
Intervention
The Intervention section documents what the clinician actually did in the session to work toward that goal.
This means naming the therapeutic approach used, not just describing the conversation. Cognitive behavioral therapy, motivational interviewing, exposure-based techniques, psychoeducation, and specific worksheets or exercises all belong here, along with any clinical reasoning behind choosing that approach for this session.
Specific, clinical language matters more in this section than almost anywhere else in the note. “Discussed coping skills” tells a reviewer almost nothing. “Used cognitive restructuring to challenge catastrophic thinking related to public speaking, including a thought record exercise,” tells them exactly what skilled clinical work happened.
Response
The Response section captures how the client reacted, both in the room and in their reported life outside it.
This is where direct quotes from clients, observations of behavior and level of engagement go. Has the client done the homework given in the previous session? Has there been resistance to an intervention?
Did they show a shift in affect or insight partway through?
Both positive and negative responses belong here. A session where an intervention didn’t land is still clinically useful information, and documenting it honestly protects the clinical record far better than a note that only ever says things went well.
Plan
The Plan section outlines the concrete next step, for this client and for the broader course of treatment.
This usually includes the focus for the next session, any homework or between-session assignments, referrals if needed, and any adjustments to the plan of care based on what the Response section just revealed.
A Plan section that simply says “continue weekly sessions” without connecting back to the Goal and Response sections is one of the most common ways GIRP notes lose their value during a chart review.
Spend Less Time Writing Therapy Notes
Stop building every progress note from a blank screen. Vozo’s AI-assisted charting helps organize session details into structured note drafts, so you can review documentation faster and focus more of your day on client care.
GIRP Note Example
A complete GIRP note for a hypothetical outpatient therapy session addressing social anxiety.
Goal: The objective driving this session is to decrease avoidance of work-related social situations and overall anxiety in group settings, with a near-term focus on initiating one short conversation per day in a low-stakes setting.
Intervention: Therapists will employ tools from cognitive-behavioral therapy to identify automatic thoughts associated with fear of judgment in social contexts. Introduced the thought record worksheet and worked through one together with the client on a recent work lunch that was stressful.
Response: Client was very involved in the thought record activity and noted the automatic thought “everyone is judging how awkward I sound. Client reported 2 of 5 conversation attempts since last session, both of which “did not feel as scary as I thought they would be. Avoidance challenges appeared more readily accepted by clients than in previous sessions.
Plan: Continue thought record practice independently before the next session, focusing on identifying automatic thoughts in real time. Increase conversation attempts to one per day. The next session will introduce a brief in-session role play to build confidence before the client’s upcoming team meeting. Reassess the anxiety rating scale at the next session.
Notice what makes this version work. The Goal names a specific, measurable target. The Intervention names the exact technique and ties it to something concrete that the client brought in.
The Response includes a direct quote and an honest, partial result rather than an inflated “great progress” summary. The Plan moves treatment forward instead of just scheduling another appointment.
GIRP vs BIRP vs DAP vs SOAP vs PIRP: Which Format Should You Use?
All five formats can produce a clinically sound, payer-compliant note. What changes is which part of the session each one foregrounds.
| Format | Opens With | Best Fit | Common In |
| GIRP | Treatment plan goal | Goal-directed modalities like CBT, motivational interviewing, and structured skill building | Community mental health, IOP, PHP, substance use treatment, CARF settings |
| SOAP | Client’s subjective report | Medical and multidisciplinary settings, including integrated behavioral health | Outpatient, integrated care, hospital settings |
| DAP | Combined data (client report + observation) | Clinicians who want assessment and clinical judgment folded into one combined section | Community MH, private practice |
| BIRP | Observable behavior | Settings where presenting behavior and symptom tracking are the primary clinical focus | Residential, IOP, group therapy, SUD programs |
| PIRP | Presenting problem | Crisis sessions, problem-focused brief therapy | Crisis services, urgent care, short-term work |
GIRP vs. BIRP
These are the closest in structure. Both share the Intervention, Response, and Plan spine; the only difference is what the note opens with. BIRP opens with the client’s behavior, meaning what they presented with.
GIRP opens with that plan objective, meaning what the session targeted. Choose GIRP when goal linkage is the priority. Choose BIRP when intervention accountability and behavioral documentation are the focus.
GIRP vs. SOAP
SOAP separates the client’s subjective report from the clinician’s objective observations, which is valuable when multiple providers need to distinguish what was reported from what was assessed.
GIRP doesn’t make that distinction; it opens with the goal and proceeds from there. Use SOAP when chart legibility across providers matters most. Use GIRP when keeping every note aligned to the plan matters most.
GIRP vs. DAP
DAP Notes is simply faster. It merges the client report and observation into one section and gets to Assessment and Plan more directly. For private-pay, low-audit practices, that speed advantage is meaningful. For Medicaid-billed care or high-review settings, GIRP’s explicit goal-linkage is worth the additional structure.
GIRP vs. PIRP
PIRP replaces the Goal section with a Problem section, starting with the actual problem rather than a plan objective. That suits the crisis or the urgent care, where the need is more urgent than the long-term goal.
Use PIRP when the session is reactive to an acute issue. Use GIRP when it’s proactive work toward a standing goal.
Related Blogs: What Are DAP Notes? A Format Breakdown for Mental Health Clinicians
When GIRP Isn’t the Right Fit
GIRP’s biggest strength, a clear tie to the plan of care, is also where it runs into trouble in a few situations.
Crisis presentations – A client in acute distress isn’t there to work on a standing goal. Forcing the session into a Goal-first structure means skipping what’s clinically relevant or writing a goal that doesn’t fit. PIRP suits this better.
Insight-oriented or exploratory modalities – Psychodynamic and person-centered work doesn’t always move toward one measurable goal per session. Forcing it into GIRP can flatten valuable clinical material into an awkward goal statement. SOAP or DAP often fits better here.
Vague or outdated treatment plans – GIRP only works as well as the plan behind it. If the plan is stale, every note inherits that gap. The fix is updating the plan first, not switching formats.
Why Goal-Focused Documentation Matters for Compliance
Utilization reviewers and payer auditors are ultimately asking one question of every note in the chart: was this service medically necessary?
The strongest possible answer to that question shows a treatment plan goal, the specific intervention delivered against it, the client’s documented response, and a plan informed by that response. GIRP’s structure surfaces that exact chain by design, which is part of why goal-driven programs and practices operating under closer payer scrutiny often standardize on it.
To be clear, no major payer mandates GIRP by name. What payers require is that progress notes connect services back to the client’s treatment plan and demonstrate ongoing medical necessity. GIRP simply makes that requirement difficult to skip, because naming that objective is the first thing you have to write.
The Most Common GIRP Note Mistakes (and How to Fix Them)
Mistake 1: Quoting a goal that isn’t in the treatment plan
The Goal section must reference an active, current plan goal. If a new topic emerged in session and you wrote a goal around it for the note, without it existing in the treatment plan, the documentation is misaligned, and that is an audit problem.
Fix: If the session revealed a new clinical priority worth documenting as a goal, update the treatment plan first, then write the GIRP note. The note always reflects the plan, not the other way around.
Mistake 2: Vague Intervention language
“Provided therapy” and “supported the client in processing emotions” do not document a billable service. They describe a conversational atmosphere. An auditor reading these phrases cannot determine what you did, why it was clinically indicated, or how it advanced the treatment goal.
Fix: Name the technique. Describe how you applied it. Connect it to the goal. If you used CBT cognitive restructuring, say which cognitive distortion you targeted, which technique you used (thought record, Socratic questioning, cognitive continuum), and what the client worked through.
Mistake 3: Response sections that read the same every session
If your Response section could be copied and pasted from Session 3 to Session 13 without anyone noticing, it isn’t documenting clinical reality; it’s documenting a template. That’s a liability.
Fix: The Response section must reflect this session. Include the screener score from this session. Include something the client said in this session. Note whether they completed their between-session tasks. Document any change, positive, negative, or neutral, since the last session.
Mistake 4: A Plan section with no specifics
“Continue treatment” is not a plan. It’s a placeholder.
Fix: Name the specific between-session task, including instructions clear enough for the client to follow without needing to contact you. Name the next session’s clinical focus. If a goal was reached or needs revision, document it and update the plan in the same sitting.
Mistake 5: Drafting notes outside the EHR
Notes written in Word documents, Google Docs, or paper forms and later copied into the EHR introduce a privacy risk, lose the audit trail, and bypass any safeguards the EHR provides. If that draft is ever saved somewhere insecure, you have a potential HIPAA incident.
Fix: Write the note in the EHR the first time. A behavioral health EHR with GIRP templates eliminates most of the friction that makes clinicians reach for a word processor.
Tips for Writing Faster, Stronger GIRP Notes
1. Write the Goal section first, every time: Make it specific enough that it could only describe this client at this exact point in treatment, not a phrase vague enough to sit on every chart in the practice.
2. Name the technique, not just the conversation: Naming the modality and the specific intervention used takes the same time as writing something vague, and it holds up far better under review.
3. Anchor the Response in something concrete: One direct client quote or a screener score takes seconds to capture and proves the session happened the way the note says it did.
4. Keep a small bank of strong example notes: Two or three on hand make the gap between a vague Goal and a specific one obvious when training a new clinician.
How an EHR Like Vozo Makes GIRP Documentation Easier
Writing a strong GIRP note takes clinical skill. Vozo’s behavioral health EHR is built to remove the friction around it.
Vozo supports customizable notes and specialty-specific templates, so a practice can build a GIRP structured template once and have every clinician working from the same consistent four-section format, with plan goals pulled forward automatically rather than retyped each session.
Built-in outcome measures like the PHQ-9 and GAD-7 can sit alongside the note, giving the Response section a measurable data point to reference instead of a purely subjective impression.
Because documentation, scheduling, and billing live in the same system, a completed GIRP note flows directly into the billing workflow without a separate handoff step.
For practices exploring AI-assisted documentation, Vozo’s AI charting tools can help draft session notes from clinician input, which clinicians then review and finalize, cutting documentation time without removing clinical judgment from the final note.
Frequently Asked Questions
1. GIRP vs. SOAP: Which is better for therapy notes?
Neither GIRP nor SOAP is universally better for therapy notes. GIRP works better for structured, goal-directed treatment because it connects interventions and client responses directly to treatment objectives. SOAP may be more suitable when clinicians need to separate the client’s subjective report, objective observations, clinical assessment, and treatment plan.
2. How does GIRP differ from DAP notes?
GIRP notes use Goal, Intervention, Response, and Plan, while DAP notes use Data, Assessment, and Plan. GIRP places greater emphasis on treatment-plan goals and the client’s response to a specific intervention. DAP combines reported and observed information into one Data section and provides a separate section for the clinician’s assessment.
3. What are the components of a complete GIRP progress note?
A complete GIRP progress note identifies the treatment Goal addressed, describes the clinical Intervention provided, records the client’s Response, and establishes a clear Plan. It should also include required encounter details such as the date, provider, service type, duration, participants, delivery method, signature, and billing information when applicable.
4. How do you write a GIRP note when the client makes no progress?
When a client makes no progress, document the outcome objectively instead of suggesting that the intervention was successful. Describe the intervention used, the client’s actual response, barriers affecting progress, and any changes in symptoms or functioning. The Plan should explain whether treatment will continue, be modified, or require reassessment.
5. Are GIRP notes accepted by insurance companies?
GIRP notes may be accepted by insurance companies when they contain all information required by the applicable payer. Insurers generally do not require the GIRP format by name. Documentation must support the service provided, its relationship to the treatment plan, the client’s response or progress, medical necessity when applicable, and required billing details.
About the author
Lara Dixit

Lara Dixit is a Senior Business Manager at Vozo Health, specializing in EHR platforms, practice management, billing, and revenue cycle optimization. She helps healthcare providers improve operational efficiency, streamline workflows, and drive sustainable practice growth. At Vozo Health, she focuses on business strategy, healthcare automation, and scalable growth for modern medical practices.









